Dr Quang Dao
Information for orthopaedic surgeons (ACL Anatomy)
The anterior cruciate ligament (ACL) is composed of collagen fibres that connects the tibia to the femur. Currently there are two popular theories to describe the anatomy of the ACL. They are the Double Bundle Theory and the Ribbon Theory.
The Double Bundle Theory
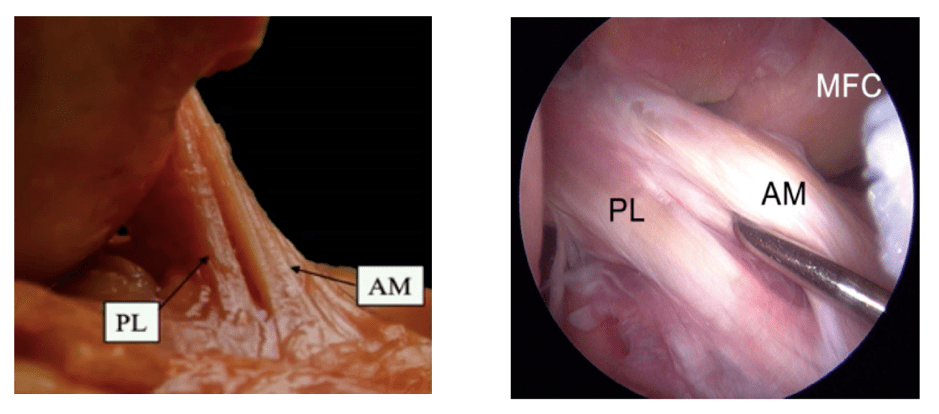
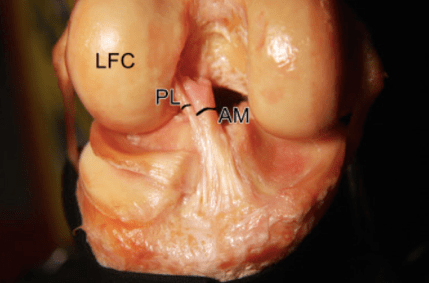
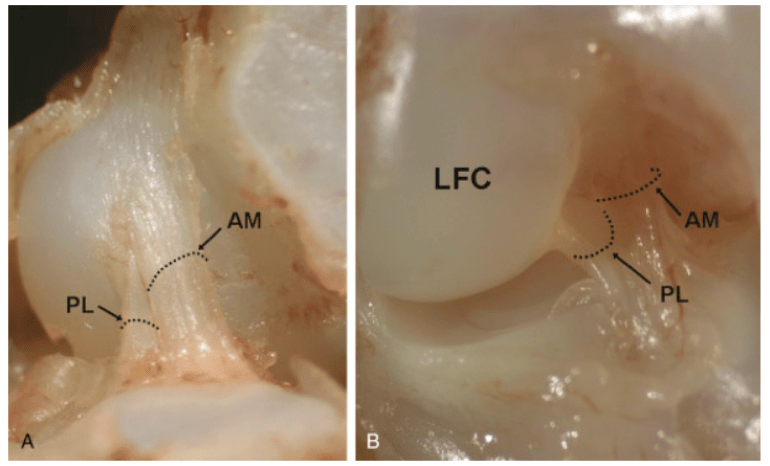
The anterior cruciate ligament (ACL) is composed of two bundles – the anteromedial (AM) bundle and the posterolateral (PL) bundle. Their names are based on their tibial insertion points. The size of each bundle varies in different individuals. The Double Bundle Theory has been popularised by Dr Freddie Fu.
The ACL is formed at about 8 weeks of gestation. The distinction of two bundles can be seen at 16 weeks gestation. The two bundles are separated by a septum. The foetal ACL is cellular and vascular.
The ACL is an intra-articular but extrasynovial structure. It is composed of dense connective tissues, mostly Type I collagen and some Type III collagen. The adult ACL is less cellular. The two bundles are separated by a vascular septum.
The ACL receives its blood supply from a synovial plexus which covers the ligament. The proximal contribution to the plexus is from the middle genicular artery. The distal contribution is from the medial and lateral genicular arteries.
Nerve fibres from the tibial nerve can be found within the ACL and in the perivascular synovium. They function in vasomotor, transmit pain impulses and act as mechanicoreceptors for proprioception.
The ACL transitions from ligament in its midsubstance, to cartilage, to mineralised cartilage and then bone at both femoral and tibial insertions. This transition allows the ACL to dissipate the forces at its insertion points.
The intra-articular length of the ACL is between 22-41mm (average 32mm). The midsubstance cross sectional area is 44mm2. It reaches about 3 times at its femoral origin and tibial insertion.
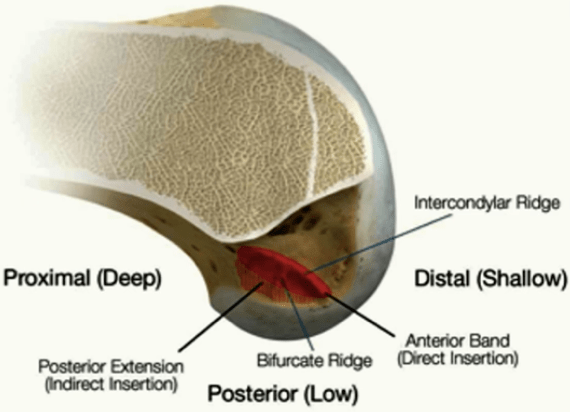
The femoral origin occupies the medial wall of the lateral femoral condyle. It is bordered anteriorly by the lateral intercondylar ridge (resident’s ridge) and posteriorly by the articular cartilage of the lateral femoral condyle. It measures 18mm in length and 11mm in width. The AM bundle is located in the proximal half and the PL in the distal half (with the knee in the extended position). The 2 bundles are separated by the bifurcate ridge. During arthroscopy with the knee at 90 degrees of flexion, the PL bundle is shallow to the bifurcate ridge and the AM bundle is deep to this ridge. The lateral intercondylar ridge can be identified arthroscopically in 88% of ACL injured knees and the lateral bifurcate ridge in 48%.
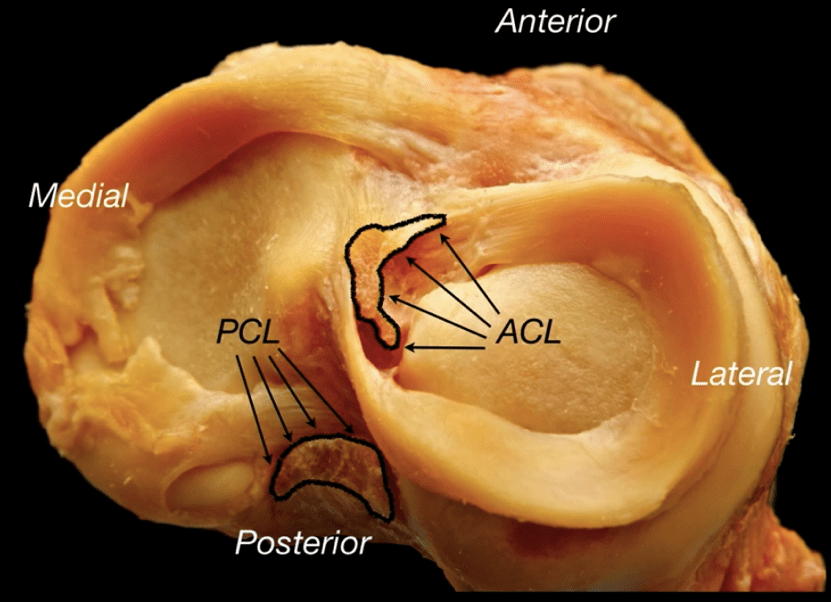
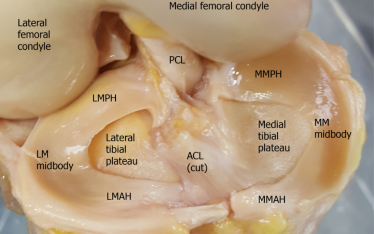
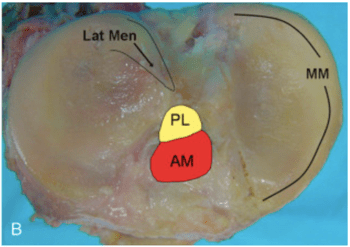
The tibial insertion is between the medial and lateral tibial spines. The medial-lateral diameter is 9-13mm (average 11mm). The anteroposterior diameter is 14-20mm (average 17mm). The AM bundle is located more anterior and medial. The PL bundle is located more posterior and lateral. The PL bundle is very close to the posterior root of the lateral meniscus.
As the knee is in extension, the femoral insertion areas of the 2 bundles are vertical to each other. In this knee position the bundles run parallel to each other.
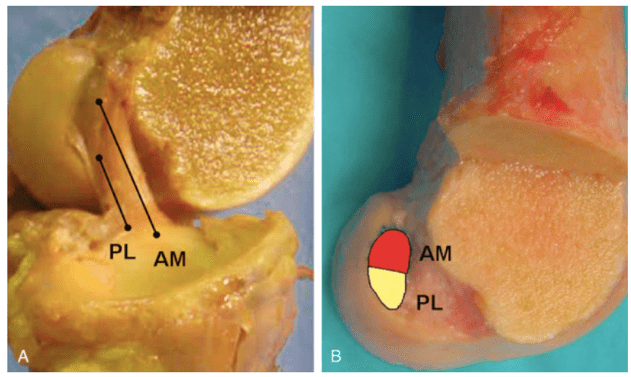
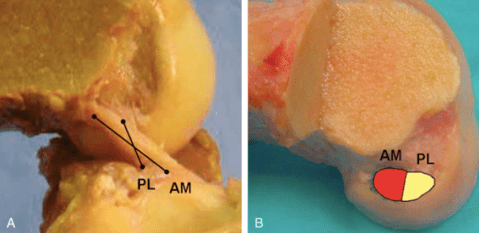
When the knee is flexed to 90 degrees, the femoral insertion sites move so that they are more horizontal with the AM bundle insertion portion more deep and the PL bundle more shallow. This relative change in femoral insertion locations causes the 2 bundles cross.
The Ribbon Theory
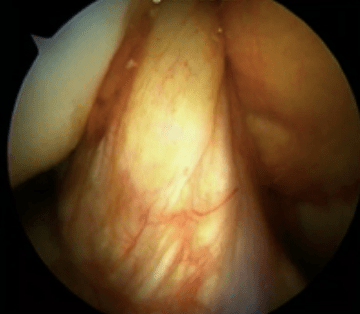
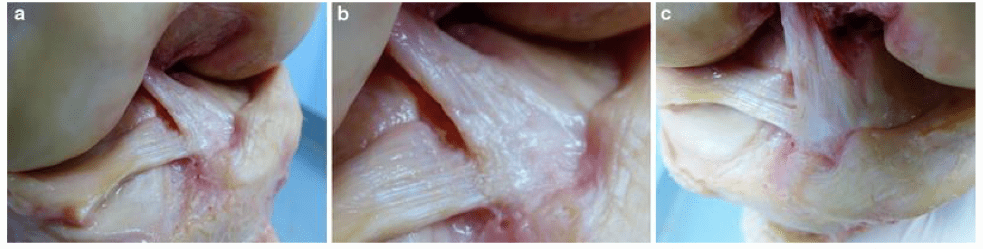
Robert Smigielski and his group popularised the Ribbon theory describing the ACL as a flat “ribbon-like” structure. Other authors have also reported similar findings.

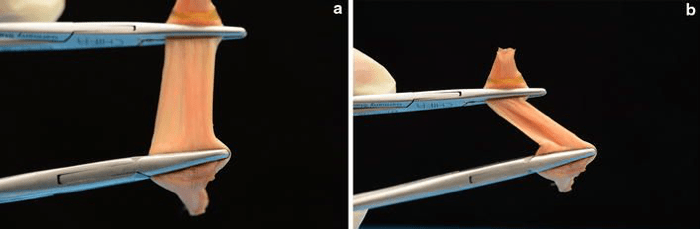
They dissected 111 fresh frozen cadaver knees, analysed them using photography, videography, CT scans, MRI scans and histology techniques. They found that the midsubstance of the ACL was flat like a ribbon.
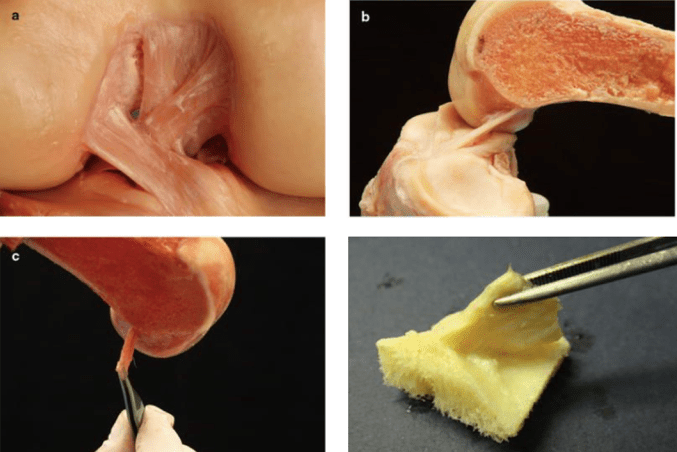
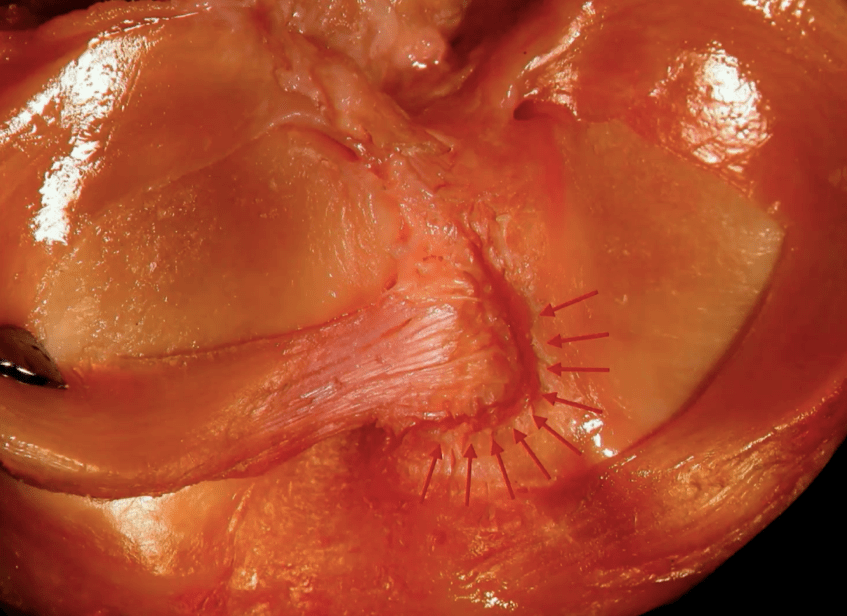
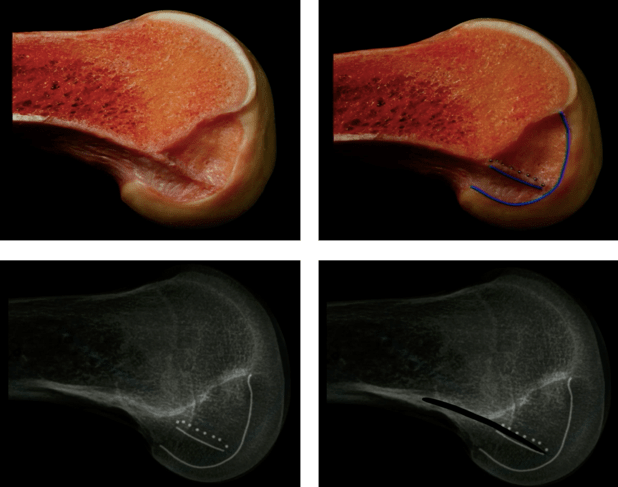
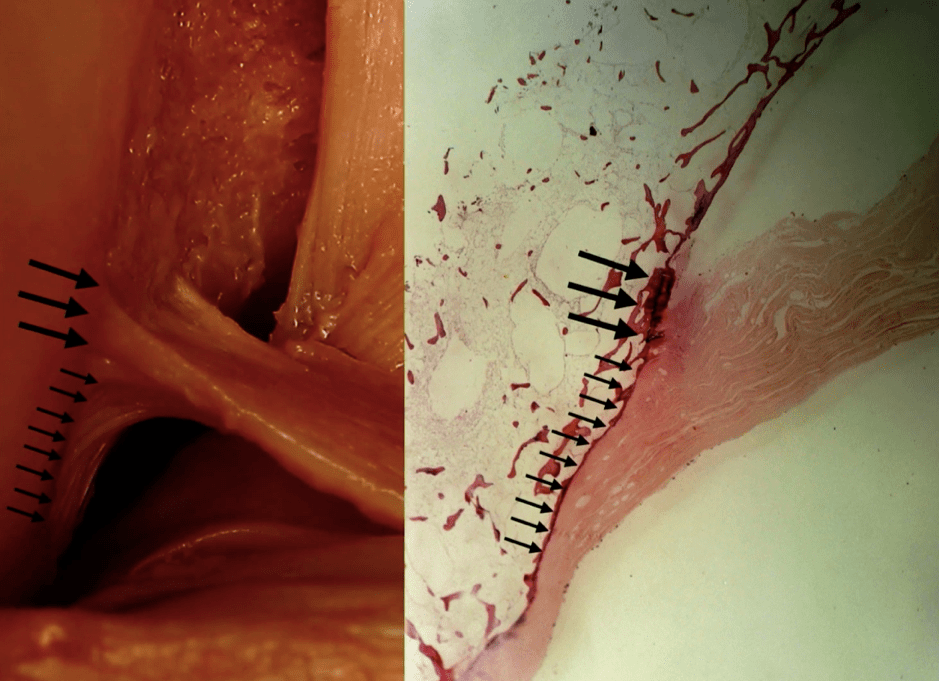
The direct fibres of the ACL insert just posterior to the lateral intercondylar ridge. This ridge is an anterior extension of the posterior femoral cortex. The indirect fibres expand and insert posteriorly towards the articular cartilage of the posterior aspect of the lateral femoral condyle.
Smigielski outlined the femoral ACL insertion area with ball bearings and radio-opaque sutures. Radiographs confirm that the direct fibres insertion points onto the lateral intercondylar ridge is a direct extension of the posterior femoral cortex.
Their dissections could not identify a separation of the ACL into 2 bundles.
They postulate that this double bundle appearance is due to the twisting of the ribbon structure as it spans from the femoral origin to its tibial insertion.
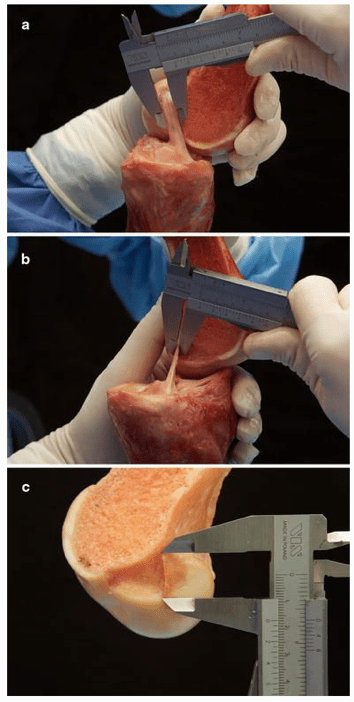
Their measurements showed
- Mean width 2 mm from femoral insertion: 16.0 mm (12.7–18.1)
- Mean thickness 2 mm from femoral insertion: 3.54 mm (2–4.8)
- Mean cross-sectional area 2 mm from femoral insertion: 56.6 mm2
- Mean width at midsubstance of ACL: 11.4 mm (9.8–13.8).
- Mean thickness at midsubstance of ACL: 3.4 mm (1.8–3.9).
- Mean cross-sectional area at midsubstance of ACL: 39.8 mm2
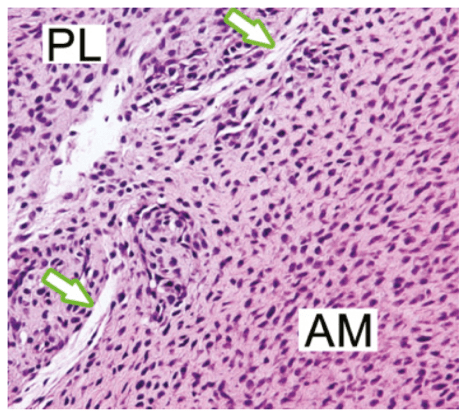
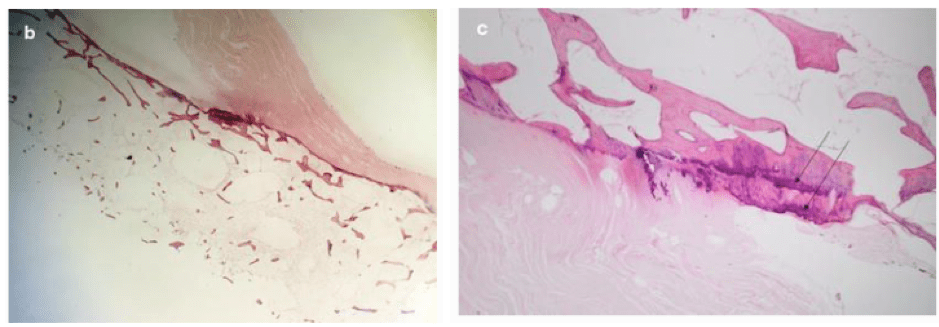
Histologic examination demontrates that the fibres are oriented obliquely to the bone surface. The bone is denser at the direct fibres insertion points (thick arrows). The indirect fibres take up a larger area towards the articular cartilage of the posterior lateral femoral condyle (thin arrows).
In another dissection study of 20 cadaver knees, Rainer Siebold et al confirmed the ribbon-like midsubstance structure of the ACL. They also described the C-shaped tibial insertion footprint. The tibial insertion runs along the medial tibial spine to the anterior border of the anterior root lateral meniscus. The centre of the “C” is the bony insertion of the anterior root lateral meniscus. In some cases, the fibres of the ACL and meniscus blend in. In other cases, they are separate.
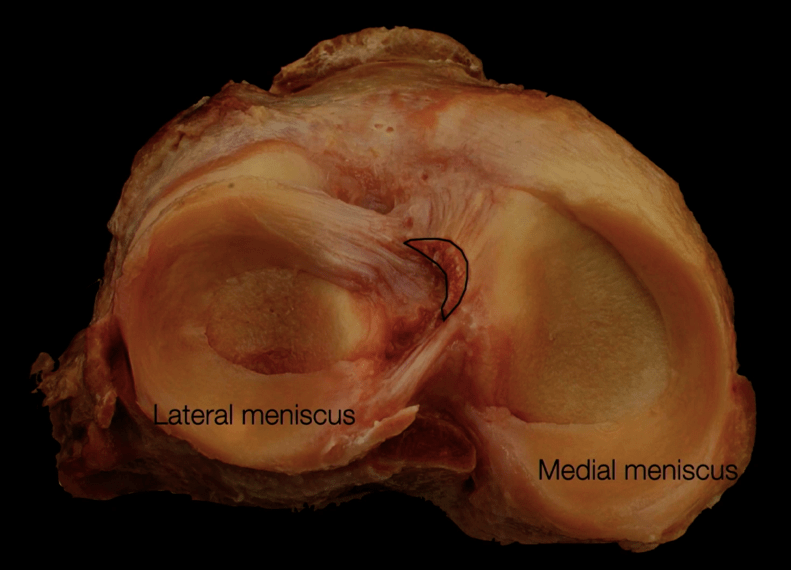
The most anterior part of the C is 9.3mm in the mediolateral direction. The central portion of the C, along the medial tibial spine is 11.4mm in the anteroposterior direction.